Last Updated: May 01, 2023
Medically reviewed by NKF Patient Education Team
About urine albumin-creatinine ratio (uACR)
The urine albumin-creatinine ratio (uACR) test measures the amount of two different substances in your urine - albumin (a protein) and creatinine.
- Albumin is an important protein normally found in the blood that serves many roles in the body. These roles include building muscle, repairing tissue, and fighting infection. It is not usually found in the urine.
- Creatinine is a waste product that comes from the digestion of protein in your food and the normal breakdown of muscle tissue. It is removed from the body through the kidneys and is expected to be found in the urine.
Healthy kidneys stop most of your albumin from getting through their filters and entering the urine. There should be very little or no albumin in your urine. If your kidneys are damaged, albumin can “leak” through their filters and into your urine. Having albumin in your urine (also known as albuminuria or proteinuria) can be a sign of kidney disease, even if your estimated glomerular filtration rate (eGFR) is above 60 or “normal”.
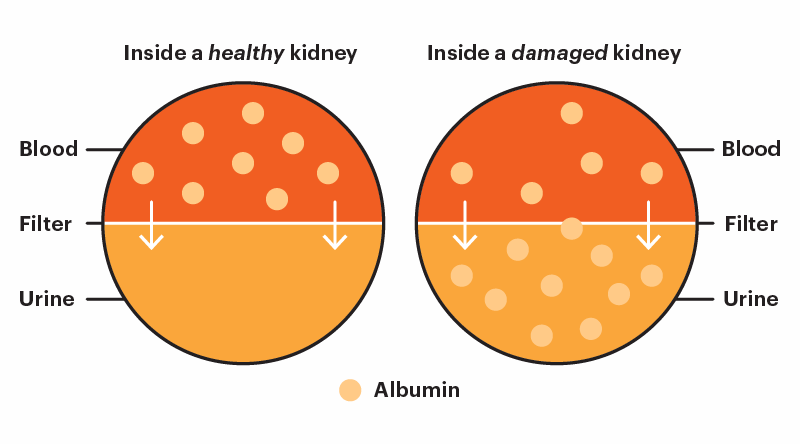
Having albumin in your urine (albuminuria or proteinuria) can be a sign of kidney disease, even if your eGFR is above 60 or "normal".
DOUBLE your impact today.
- Equip patients and families with knowledge, resources, and access to high-quality care.
- Advocate for policies that address disparities and prioritize kidney health for all.
- Fund research and technology to advance early detection, improve treatment, and expand transplant access.
Types
There are four different types of tests available to test your uACR. The quantitative uACR test is the most preferred initial test for adults at high risk for kidney disease because it offers the most precision while also being convenient. The National Kidney Foundation supports semi-quantitative uACR testing for adults at increased risk for kidney disease when access to quantitative testing is limited. Semi-quantitative tests offer less precision but more convenience since they can be done at home or in a doctor’s office.
Purpose
The uACR is an important test for identifying kidney damage, in addition to the eGFR test. Albuminuria (having albumin in your urine) increases your risk of kidney failure and cardiovascular disease (heart attack or stroke). It can also decrease your life expectancy if left untreated. Kidney disease usually does not show any symptoms until the later stages of the disease – so it is important to have a uACR test done at least once a year if you have any of these risk factors:
- Diabetes
- Hypertension (high blood pressure)
- Cardiovascular disease (history of heart attack or stroke)
- Heart failure
- Family history of kidney disease, kidney failure, or dialysis
- Increased body weight (especially if your body mass index or BMI is over 30)
- Smoking or other use of tobacco products
- Over the age of 60
Albuminuria (having albumin in your urine) increases your risk of kidney failure and cardiovascular disease (heart attack or stroke). It can also decrease your life expectancy if left untreated.
Before the test
Ask your health care professional if there are any special instructions to follow.
For tests that require a “spot” urine sample, an early morning sample (at least 4 hours without using the bathroom) is preferred but not required. Make sure to drink enough water the day before the test to avoid dehydration and be prepared to make urine during your appointment.
Avoid intense exercise in the 24 hours before your test - this can cause a temporary increase in your uACR. Similarly, you may need to reschedule your test if you experience any of the following events in the 24 hours before your test as they can also interfere with the test and lead to a false positive result:
- Fever and/or infection
- Heart failure exacerbation (flare-up)
- Urinary tract infection
- Urinary or menstrual bleeding
- A sudden and dramatic increase in your blood pressure or blood sugar
You may also be asked not to eat any meat the day before the test. There is a possibility that it can increase the level of creatinine in your urine and affect your results, although this is not very common.
During the test
Specific instructions may vary by testing center - be sure to follow the instructions provided to you by your healthcare professional or laboratory staff.
In general, this test uses the “clean catch” method to collecting your urine sample. This method includes the following steps:
- Wash your hands with soap and water.
- Clean your genital area with a cleansing wipe.
- Urinate into the toilet for a few seconds and then stop the flow.
- Start urinating again, this time into the container. To avoid contaminating the sample, do not let the inside of the container touch your body.
- Collect at least 1-2 ounces (30-60 mL) of urine in the container. Most containers have markings to show you how much is needed and when you can stop.
- Finish urinating into the toilet.
- Put the cap on the container and return it as instructed.
Results
The uACR test checks for how much albumin and creatinine is in your urine sample, and then compares the numbers to each other. You may see many numbers from this test on your lab report – focus on the result that has the word ratio in the name. For example, the name on the report may be “alb/creat ratio”, “albumin/creat ratio”, or “albumin/creat ratio, random urine”.
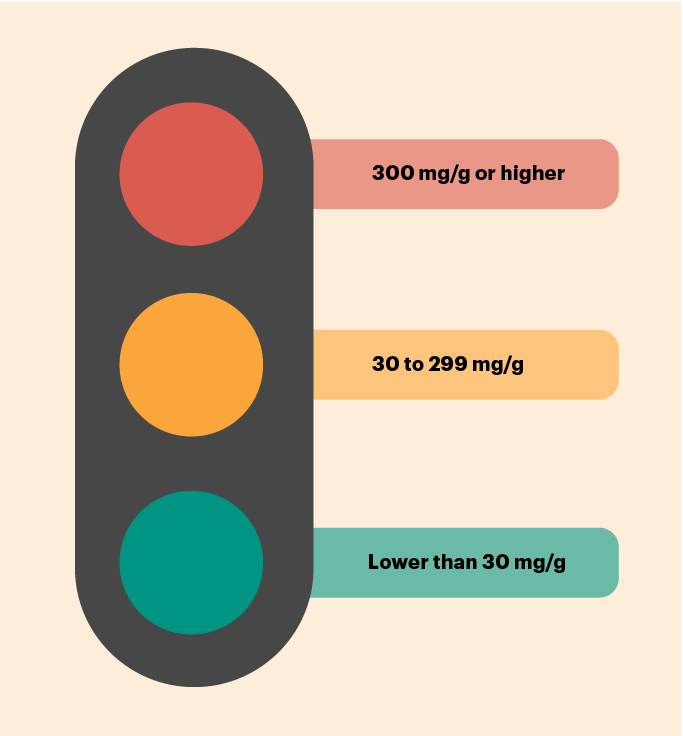
Your uACR results help describe the degree of albuminuria (proteinuria) you may be experiencing, if any. A lower number is better for this test, ideally lower than 30. A value of 30 or higher suggests you may be at a higher risk for kidney failure, a cardiovascular event (heart attack or stroke), heart failure, and even a shorter life expectancy (early death). The higher your number, the higher your risk.
What to do next with your results depends on what your number is. It’s important to emphasize that this test often needs to be repeated one or more times to confirm the results. Decisions are rarely made based on the results from one sample.
Follow-up testing
Your healthcare provider will advise you on how often to do this test. The recommended frequency ranges from once a year to 4 or more times per year depending on your specific condition.
Recommendations for how often you should do follow-up testing depend on your initial uACR results, your eGFR results, and whether you have been diagnosed with kidney disease.
If you completed a semi-quantitative or urine dipstick test and the results are positive (show albumin in your urine), follow-up testing with a quantitative uACR is recommended.
Your uACR results help describe the degree of albuminuria you may be experiencing, if any. A lower number is better for this test, ideally lower than 30.
Questions for your healthcare team
- When was the last time I had a uACR test completed?
- Should I have my uACR test repeated to confirm my results?
- Are there any special instructions I should follow to prepare for my uACR test?
- Do I have kidney disease based on my eGFR and uACR results?
- What do my uACR results mean in the context of my overall health?
- [If you did a semi-quantitative test] Based on my results, should I complete a follow-up quantitative test?
- What steps can I take to lower my uACR and risk of complications?